Injuries and their Tissue Mechanics 2/12 (Warning: Prosected Images)
Injuries and their Tissue Mechanics 2/12 (Warning: Prosected Images)
26 research papers and 639 human lower limb studies the anatomy of the sciatic nerve, its motor branches and motor entry points appears to be more of a heterogeneous formation
Personal Trainer to Clinical Anatomist
When I worked at a Personal Trainer, with a successful client base, I quickly learnt that my anatomy education had been bias towards understanding the principles of anatomy through classic anatomy ‘book’ and it’s application to exercise rehabilitation. I personally believed there was a ‘missing link’ in my anatomy knowledge. In 2010 I begun my Clinical Anatomy Qualification at Keele University, Staffordshire. I spent three years dissecting and exploring our human form and documented the anatomy in the books we read was only present in 56% of the population – the rest have a variety of forms.
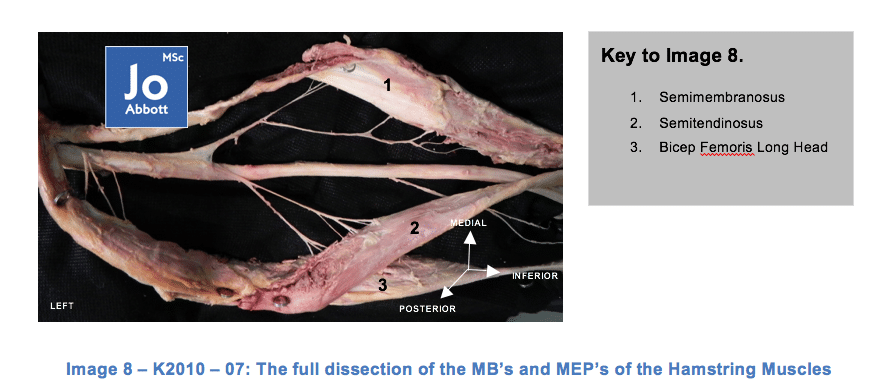
For my final exam I chose to dissect the path of the sciatic nerve (SN); observe its anatomical relationship with the piriformis muscle (PM) and to measure; the diameter of the SN as it exits the greater sciatic foramen, the motor branches (MB’s), motor entry points (MEP’s) innervating the hamstring muscles and to observe and measure the bifurcation point of the tibial nerve (TN) and the common peroneal nerve (CPN). The ‘motor branch’ is defined as the point where the branching nerve leaves the perineurium of the sciatic nerve and the ‘motor entry points’ are where the motor branches pierce the muscle belly (Seidel et al. 1996).
Sciatic Nerve Anatomy
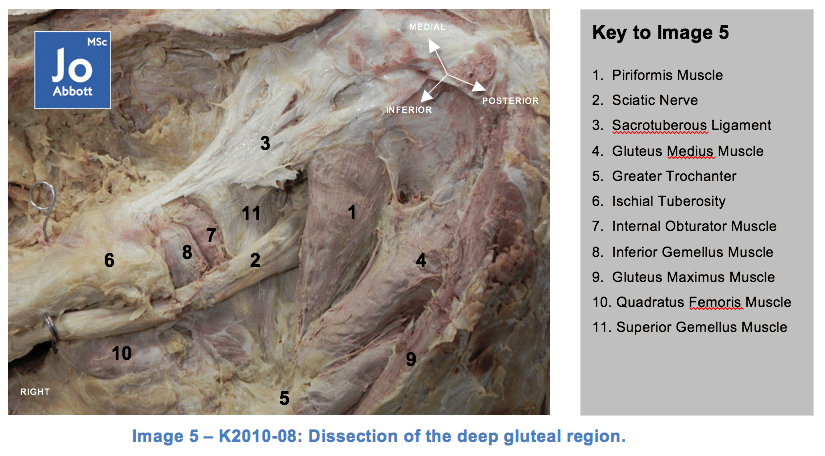
The sciatic nerve is the largest single nerve trunk in the body (Babinski et al. 2003). The sciatic nerve passes through the inferior aspect of the gluteals and descends into the posterior compartment of the lower limb, supplying motor and sensory innervation to the skin, and muscles in the legs and feet (Vloka 2001). Formed in the pelvis L4, L5, S1, S2 and S3 spinal roots considered the continuation of the plexus; the sciatic nerve traverses the greater sciatic foramen crossing the anterior third of the foramen on the anterior surface of the piriformis muscle (Güvençer et al. 2008).
Bifurcation of the sciatic nerve into the tibial nerve and common peroneal nerve may occur anywhere between the sacral plexus and the lower part of the popliteal space (Sunderland & Hughes, 1946; Nizankowski et al., 1972; Abbott, 2012). Both tibial nerve and common peroneal nerve innervate the hamstrings; the common peroneal nerve also innervates the dorsal surface of the foot, whilst the tibial nerve innervates the plantar surface of the foot (Zehr et al, 1998). The diameter of the sciatic nerve as it leaves the foramina varies from 5mm up to 17mm (Heinemeyer & Reimers, 1999; Güvençer et al. 2008; Abbott, 2012).
In summary, from a total of 26 research papers and 639 human lower limb studies the anatomy of the sciatic nerve, its motor branches and motor entry points appears to be more of a heterogeneous formation rather than a precise location (see image below).
Piriformis Muscle Anatomy
In the Sixteenth Century an Italian Professor at Padua, Spigelius, was the first anatomist to name the piriformis muscle, meaning ‘pyramid‘. It is important to note that as far back as 1900’s the action and function of the piriformis muscle has been under much debate as has its anatomy.
The piriformis muscle is one of six deep small hip external rotators. It is uppermost to the gluteal muscle group and imperative to the arrangement of the vessels and nerves in the buttocks. Key to understanding this muscle we must first become orientated with its anatomical features and functions; then later we shall be examining the literature with regards to the variety of its morphology, histology and the significant implications these have.
The piriformis muscle largely fills the greater sciatic foramen, through which the branches of the sacral plexus and branches of the internal iliac vessels to the gluteal and pudendal regions leave the pelvis; therefore, the vessels and nerves that enter the buttock necessarily are closely related to this muscle (Williams 1999). Its proximal attachment starts at the anterior aspect of the second to fourth sacral segments and extends between the lateral to the anterior sacral formina.
From its additional attachment on the gluteal surface of the ilium, near the posterior inferior iliac spine, and the pelvic surface of the sacrotuberous ligament it then feeds out of the pelvis through the greater sciatic foramen. Bouisson arcade is a lower convex fibrous arcade stretched from the anterior edge of the greater sciatic notch to the sacroiliac joint, immediately above the upper edge of the piriformis muscle (Paturet,1951). Its fibres continue downwards laterally and forwards narrowing into a rounded tendon to attach to the medial side of the greater trochanter of the femur.
The innervation of the piriformis muscle comes from the piriformis nerve, from the sacral plexus L5, S2, but mainly S1. (Palastanga et al, 2006). It leaves the pelvis through the greater sciatic foramen and below through or above the piriformis muscle before extending distally between the greater tuberosity of the femur and the ischial tuberosity of the pelvis into the lower extremity. The Arterial Supply comes from the superior and inferior gluteal artery along with the lateral sacral artery.
Next Blog: “How does this system go wrong”?
How does this anatomical relationship become compromised?
How does this affect active daily tasks?
What injuries can be sustained to this area?
What symptoms ‘drive’ the diagnosis of ‘sciatica’?
There are so many mechanisms involved in squatting, some of these mechanisms are fundamental to the human design, others blow off the cobwebs and allow us to keep moving safely and efficiently. Reducing squatting exposes the joints to premature aging; knees, hips, ankles, spine, and pelvis.
I know, crazy right? I must be mistaken? It has to be some kind of black magic? I'm pain-free because of some other factor? It must be psychosomatic?To be honest, I have heard it all now. What's important? My wrist is pain-free enabling me to get back to a normal life after 2 years of pain!
“Personally I feel fantastic and it is all down to you and your amazing healthy programme especially the BodyMOT Lifestyle & Biomechanical Assessment. I...
By volunteering as testers and participants in various experimental and inter-tester reliability studies allow you be a part of the latest clinical research in...
Artwork Only This banner (pop-up or eyelets) has been designed for the Therapist wanting to reduce any perspective, parallax or subjective errors within their...




0 responses on "Injuries and their Tissue Mechanics 2/12 (Warning: Prosected Images)"